LONG READ
What is at stake when the US Supreme Court takes on Obamacare?
Ahead of a key court hearing on the constitutionality of the Affordable Care Act, we look at what it could mean for Americans.
Published On 9 Nov 2020
|
Updated:
11 Nov 2020
05:57 AM (GMT)
On November 10, the Supreme Court of the United States will hear a new case against the Affordable Care Act (ACA), the signature legislation of Barack Obama’s two-term presidency.
It will be heard by a court that is more conservative than Americans have known for generations, with its newest judge Amy Coney Barrett rushed into a vacant seat just days before the divisive presidential election. This tipped the balance of the already conservative-leaning nine-member court to a much more weighted 6-3 split in their favour.
Keep reading
list of 4 itemsDeadly Sahel heatwave caused by ‘human-induced’ climate change: Study
Woman, seeking loan, wheels corpse into Brazilian bank
UK set to ban tobacco sales for a ‘smoke-free’ generation. Will it work?
The case, California v Texas, which deals with the constitutionality of the 2010 ACA (commonly known as “Obamacare”), is the latest salvo against a complex, intricate law that is loved, hated and misunderstood in the US, and that touches the lives of almost everyone in it.
The hearing comes just in the wake of Donald Trump losing the presidential election – even as he refuses to concede – while nearly a quarter of a million people have died from COVID-19, and as millions of American citizens have lost their jobs and their health coverage.

Healthcare in the US: A short history
Since the second world war, most Americans have known that good health insurance is tied to a good job.
But in the 1960s, two government options were created by the Lyndon Johnson administration: For Americans over 65, there was Medicare, a programme that has long been popular and difficult to cut due to its wide bi-partisan reach (everyone gets old).
And for the poor, there was Medicaid, which is administered individually by states, resulting in wide variations in who is eligible. In some states, for example, children were only covered by Medicaid if their parents earned less than half of what would put a family of three on the federal poverty line (approximately $9,000 a year at the time), while in other states, with more progressive policies, children would be covered if their family’s income was $55,000 for a family of three.
Despite these limited government options, health insurance was understood as a private enterprise, and across the insurance market, plans were shaped by the demands of hospital networks and providers.

By the 2000s most insured Americans were covered by a private healthcare plan they chose through their workplace. In 2008, a family would, on average, pay $12,300 per year just to own a plan through their workplace, with additional co-payments for services, medicines, and therapies on top of that. That average premium also varied widely between states.
For those who wanted something else, or for the wealthy, self-funded private medical plans were available. In 2009, someone buying individual non-employer health insurance would pay about $3,600, or $7,000 if it also covered their family, but pay much higher deductibles for medical services. Many of these plans were not as comprehensive as employer-backed options.
For most insured people (59 percent of employee plans and nearly 90 percent of individual plans) there were lifetime caps on how much total coverage a provider would pay for. After that cap – sometimes one or two million dollars – was reached, insurers would stop covering, even if the treatment continued.
Hitting such a maximum might seem unlikely, but for someone receiving specialised treatments, or managing the care of a very sick premature baby, those costs could be exceeded within a few years or less, and the patient would be left to cover the remaining costs. A long-term stay in the ICU could leave a family in financial ruin.
Insurance companies considered future health complications liabilities, and charged higher costs or did not sell policies to people with so-called pre-existing conditions, affecting more than 100 million Americans in 2010. A pre-existing condition could be asthma, a family tendency towards high blood pressure, or a likelihood the patient would develop cancer.
Women are statistically more likely to develop diabetes and cancer than men and were disproportionately uninsured, in part due to the pre-existing conditions loophole. In 2010, 20 percent of women aged 18 to 65 did not own health insurance.

Black and Hispanic Americans were also insured at lower rates. In 2010, 13 percent of white working-age Americans, 20 percent of Black Americans and 33 percent of Hispanic Americans were uninsured. Among those who did have a plan, higher numbers of Black and Hispanic Americans were receiving Medicaid, which often delivered lower-quality care options. People of colour in the US are more likely to live in low-income families without access to an employer-sponsored option, and most private plans were out of reach. As a result of this lack of health insurance – along with other barriers to care – these groups are also less likely to receive preventive care, diminishing overall health outcomes.
For the uninsured patient walking into a clinic, price vertigo could quickly strike. With most doctors and nurses unable to tell a patient how much the eventual cost of a medical service would be, they would have to decide whether to receive treatment before knowing if they could afford it.
Typically for an insured patient, a medical provider would submit documentation of a medical service – a physical exam, a blood test, an MRI, for example. The insurance company negotiates reimbursement with the health network and the patient gets the bill after treatment has been delivered. Depending on how much their plan covers, the patient may pay a portion.
Meanwhile, medical interventions in the US have become more state-of-the-art, more expensive, and more common.
By the early 2000s, health spending accounted for roughly one-sixth of the US economy, the largest share in the world, but only about 85 percent of Americans had health insurance. Many of the millions of families left out were an injury or illness away from dire financial consequences.
The cost of care
Marleny, who prefers that Al Jazeera use only her first name, was one of the millions of uninsured. She lives in Framingham, Massachusetts, and is a single mother of 9-year-old twin girls and a 20-year-old daughter. She is an immigrant from Guatemala and used to live in California, where she had a basic insurance plan sponsored by her employer while she was pregnant. In addition to her premium, she paid $30 for a doctor’s visit and $500 for each birth.
When she moved to the Boston area in the cold winter of 2014, all of her daughters fell ill with bronchitis. She was scared to take them to the hospital.
“I waited a week to take them to the hospital. My daughters had a lot of fever and coughing, and I noted they were losing weight. My mother said, ‘You need to take them’,” Marleny explained in a phone interview.
The family of four was living in a single rented room and their car had not yet arrived from the west coast. But with her daughters’ conditions worsening, Marleny knew she had to do something. She borrowed a car from someone she knew, packed the twins, then two years old, and her older daughter into it and drove.
There were two things Marleny did not know when she walked into the Emergency Room at Metrowest Medical Center: that Massachusetts did have some state coverage plans available for low-income people, and that the first provisions of the ACA were just coming into effect. She thought of walking back out into the cold.
“I was scared that I might get a high bill. I told them I don’t have health insurance here, and I don’t know how much this will be.”
Her story mirrored others playing out in ERs across the US. She would soon discover that a reform bitterly fought on the national level was at that moment becoming available. Too concerned about her girls’ health to leave, she decided to stay.

Attempts at health reform
During his term, President Bill Clinton tried to reform the healthcare system – but failed.
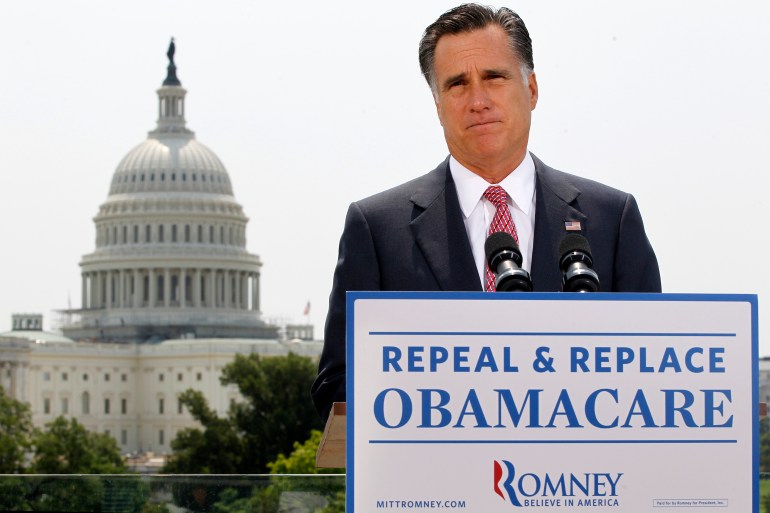
Then, in 2006, Republican (then-governor) Mitt Romney succeeded in delivering Massachusetts, a wealthy liberal-leaning state, a form of universal coverage in which everyone was obligated to buy insurance. State-funded options were available to those making up to 300 percent of the figure that would put someone on the federal poverty line, and at-cost individual plans were regulated and sold in streamlined marketplaces. The reform was seen as radical as until that point no state had passed a plan compelling people to buy health insurance.
When Obama debated John McCain on national television ahead of the election in 2008, he said healthcare spending was a burden on the American people and vowed to tackle it. At the time, millions were out of work and hence health insurance, due to the “Great Recession”. McCain said he would solve the problem by sending a $5,000 tax credit to the average family, which they could use to pay for health costs (at that point, the average yearly premium for a family was more than $10,000). McCain said Obama’s plan would be so limiting that it would leave “Joe the plumber”, a made-up potential user, without any plan at all.
Obama was swept into the White House with a strong mandate, and his team set out to invest their political capital directly in the divisive issue.
“Both the politics and the substance of health care were mind-numbingly complicated,” the former president writes in his new memoir, excerpted by the New Yorker on October 26, 2020. “When I think back to those early conversations, it’s hard to deny my overconfidence,” he recalled.

Democratic lawmakers drafted a 900-page bill containing hundreds of provisions. They hosted dozens of bipartisan meetings and held hours of public hearings with 200 witnesses. Senators from the Finance Committee grilled representatives from the health insurance industry, conservative think-tanks, interest groups for retired Americans and state regulators.
“A single provision tucked inside the bill could translate to billions of dollars in gains or losses for some sector of the health-care industry,” Obama reflected. It was early 2010 and the White House, the House of Representatives, and Senate were all controlled by Democrats. When it was clear that no Republican would support any law that reformed the health sector, the politicians pushed it through in a rare late-night holiday vote on December 24.
Obamacare’s bold approach
The ACA’s bold idea was to get more healthy Americans to own health insurance. This, the administration believed, would put more money into the insurance market and lower costs for everyone. The authors did it by introducing the “individual mandate”, a penalty for those who stayed uninsured, administered by Congress. Anyone who did not purchase a private plan would have to pay a fee to the Internal Revenue Service. Critics raged that the federal government was forcing them to buy something they did not want.
The ACA then clamped down on insurers by making them offer better individual plans for those without employer-sponsored options. It stopped the pre-existing condition loophole. It required insurers to include basic essentials such as emergency services, pregnancy and maternal care, and substance abuse treatment, many of which had been out-of-pocket extras before.
The law required these new individual plans to be sold in transparent marketplaces run by states, which would only offer plans that were vetted. Separately, the law dramatically expanded the free health coverage programmes for the poor and the elderly – Medicaid and Medicare – which had always missed millions who did not qualify according to their state’s criteria.
Lastly, the law invested billions in research for innovations to improve how health is paid for, and quality of delivery.
Don Berwick, a Harvard-educated paediatrician, had studied the quality of care for 30 years when he was appointed by Obama to lead this particular expansion in 2010.
“I told my staff three questions for any proposal: How would this improve care? How would this improve people in dire straights? How would this help reduce costs overall?” he told Al Jazeera.
Berwick developed plans to expand the free services and prepare the state marketplaces for launch, before resigning 18 months later due to his recess appointment. He had been criticised by Republicans after saying Britain’s NHS, a government-paid system, could be an example for the US. Opponents, like the Republican senator from Wyoming, said his approach would ration care. Dr Berwick vigorously refuted that accusation. Berwick, who has long argued for healthcare delivery to be a government responsibility, is now president emeritus of the Institute for Healthcare Improvement.
“We don’t have evidence that market forces yield improvements that we’re after. Market induces competition instead of cooperation … The market system will not encourage [knowledge sharing] … Market systems tend to lead to behaviours that favour providing services to people with more money and not people with less money. We need exactly the opposite approach,” he told Al Jazeera.
Republican lawmakers and judges took aim at the ACA from multiple angles and, in 2012, Obamacare was challenged in the Supreme Court. The National Federation for Independent Businesses (NFIB) and 26 states argued the ACA forced small business owners to buy insurance for their employees, hurting the businesses. The court did not agree, but it did transform the ACA by declaring the individual mandate was a tax, not a fine. The change was subtle but would open an opportunity for that tax to be reduced by Congress.
The justices also ruled that the decision to expand Medicaid would be left to individual states. A dozen mostly southern states immediately stopped the expansion, leaving millions without promised insurance options. The NFIB said the “constitution has been undone”.
After more than three years of preparation, the ACA became active in 2014.
More than just crisis care
Sitting in the emergency room that January, Marleny knew her girls were too sick to leave untreated. A member of the staff told her not to worry, there were plans for her. One of the new advantages of the ACA was same-day enrollment, shrinking a process that had previously taken up to 45 days. The girls were prescribed antibiotics and sent home. Her family would need emergency services several more times that winter, but Marleny was now covered, as were her daughters.
She started to think of healthcare as more than something for a crisis. Marleny began visiting her own doctor regularly, going for mammograms and other preventive services, which were free.
“Thank God we have this programme,” she said. “If not, I don’t know what we are going to do. A lot of families like mine don’t have the money to pay for health insurance.”
Marleny is not unemployed. She works as an administrative assistant at an NGO that provides housing help to people in Massachusetts, making about $2,500 each month. She says her employer-provided plan costs $600 a month for the premiums alone, too expensive for her to afford. Her income, near the poverty line, makes her eligible for the subsidised plans Don Berwick helped expand. Her ACA-insurance costs just $45 per month; a visit to the doctor costs $18, medicine for the children costs her a few dollars.

Marleny’s insurance is available because Massachusetts receives federal money for people in her situation. Health Care for All, an NGO in the state, helps her navigate the process. For many years Hannah Frigand, the NGO’s director of education and enrollment services, received phone calls from people eager or desperate to secure a coverage plan.
“We hit a peak when the ACA was implemented,” she told Al Jazeera. Calls nearly doubled as the law was passed, and again when it was implemented four years later. Thousands of people had been waiting for better coverage.
Trump and the case against Obamacare
Donald Trump criticised the ACA in his very first speech as a candidate, calling Obamacare “a disaster”. He claimed, citing anecdotes, that patients would lose their health coverage, doctors would quit, and the health consumer would be stuck with ballooning payments. When he spoke in 2015, about 17 million new working-age Americans were insured who previously had not been before the law. The average family premium for employer-sponsored insurance had indeed gone up, as it had every year before and continues to today, but the cost of individual plans was falling. In his first day as president, Trump issued a broad executive order for government agencies to scale back as many parts of the ACA they could.
With control of both Houses of Congress in 2017, Republican lawmakers pushed forward bills to repeal and replace Obamacare. Their “skinny” version lowered the individual mandate to zero dollars, leaving the rule with no penalty. But their replacement preserved much of the ACA’s popular parts like coverage for pre-existing conditions, for children up to 26 years old under their parents’ plans, and the expansion of Medicare.
In an after-midnight vote on July 28, 2017, Republican Senator John McCain, who had been facing months of aggressive criticism from President Trump and who had just been diagnosed with a brain tumour that would take his life a year later, walked to the podium and held his thumb down for the cameras to see. The ACA would continue.

Nisha Kurani studies the law and its effects at the Kaiser Family Fund (KFF), an organisation that tracks the medical insurance industries. In a phone interview, she said the loss of the individual mandate has, paradoxically, not had the impact many feared.
“Early on there were concerns that the market would destabilise. But that hasn’t happened. Premiums in the past years have gone down. Healthy people have not left the market as was predicted. And the financial health of insurers has dramatically improved since the early years of the ACA. We’ve seen that the marketplace has stabilised.”
At the start of the Trump presidency, 20 million new Americans were insured by the expanded programmes. The gap between uninsured Black and white Americans fell by four percent, and that between uninsured Hispanic and white Americans fell by over nine percent. The number of uninsured women halved in two years.
The White House under Trump pushed for many parts of the ACA to be undone. Obamacare blocked a type of short-term insurance option sold across states that had often driven consumers into medical debt: The user would buy one, undergo a treatment, and find it was not actually covered. The ACA limited these plans to 30 days, the Trump administration extended that to a full year with the option of renewal.
Watchdog organisations have documented how the websites for state marketplaces have been closed for hours or days during enrollment periods, due to “maintenance”, preventing people from finding health plans. Funding for public messaging about health insurance has been reduced. States have seen their waivers for innovation programmes cut. Some states have imposed work requirements for Medicaid, demanding that people who receive the subsidised coverage for the poor prove that they are employed, even though studies have shown that most on the programme already are working or have a good reason such as disability not to.
In one stirring example, money intended for medical research and other services was moved by the White House’s Health and Human Services director to pay for the detention of migrant children. These cuts have made a difference: the uninsured rate has been growing slowly since its 2016 low, creeping up by a few million people.
The new challenge
This Tuesday, November 10, the ACA will again be challenged at the Supreme Court.
Texas, 18 other – traditionally Republican-led – states, two individuals and the White House say the whole law must be thrown out because the individual mandate is zero, “a law that does nothing”, the case says. The justices will first decide whether the two sides have what is called “standing”, they will ask whether the individual business owners have been injured by the ACA. It will be a difficult argument, as there is no penalty for not buying insurance. If the plaintiffs do not have standing, the case will be rejected.
The justices will then decide whether the ACA would have been written and passed had it been known at the time that the individual mandate would be unconstitutional. If the answer is yes, the individual mandate could be sliced off the law, or severed, leaving the rest intact. The court could rule that both the individual mandate and the protections for pre-existing conditions are unlawful, but leave states to decide which subsidies and other parts to preserve.
If the court agrees with the federal decision made in Texas and strikes down the law, the impact would be profound. It is estimated that 23 million people could lose their health coverage (20 million who gained it plus another 3 million who have had to find new plans since the start of the pandemic). States that have taken full advantage of the subsidies of the ACA would lose those funds in their budgets. Massachusetts may have to cut programmes that prevent Marleny from worrying whether rent, food or health costs come first.
“Pulling away the ACA would be, I think, a disaster for millions of people in this country,” Berwick told Al Jazeera. “They would be left high and dry, angry, their costs would soar … it’s hard to imagine the ACA being pulled away at this point without severe dislocations.”

All eyes are now on Amy Coney Barrett, the newest justice. She was clerk to the court’s most famous recent conservative justice, Antonin Scalia, who dissented both previous healthcare rulings. Justices are not often public speakers, so Barrett’s verbal record has been combed over looking for clues as to how she could rule. She has said she supported the dissent in a previous case against the ACA – but as a law professor, not a judge.
In her confirmation hearings, she said the Supreme Court tends to rule in favour of severability, keeping most of a law if a part can be chopped off. Whether or not California v Texas prevails, this is unlikely to be the final case to challenge the ACA.
In 2020, the Affordable Care Act is still (mostly) law, and it is as popular as it is divisive. Most Americans want the whole ACA to stand, though most Republicans want to see it repealed. More than 90 percent of Democrats and two-thirds of Republicans do not want to see protections for pre-existing conditions disappear. Critics like the Cato Institute and Heritage Foundation write that the law is too expensive for both the government and for beneficiaries, and too limiting for the American consumer.
Under the ACA, more people are insured. Costs for individual insurance buyers have fallen, but costs for insurance through work have grown. Expanded Medicaid services are credited with saving tens of thousands of lives, protecting essential workers during the pandemic, and even slowing eviction rates in high-enrollment areas (one study suggested that low-income users were less frequently forced to choose between paying rent and paying for health costs).
The US is a country that has incredible health resources, but mixed outcomes. Measured against comparable nations, the US has better outcomes for its cancer patients and worse outcomes for maternal mortality, according to Kurani at KFF. Healthcare is a work in progress.
Berwick advocates taking a long view.
“If we can take a breath as a country and depoliticise this, there’s a lot to be learned. ACA is not a perfect law. It has many elements that could be better.
“I think the ACA, even as weakened now, can and should survive … Then we have to remember – it still left 30 million uninsured, so there’s work yet to do.”
–
Update, November 11, 2020: In the hearing on November 10, conservative Justice Brett Kavanaugh spoke in favour severing the individual mandate. “This is a fairly straightforward case for severability under our precedents, meaning that we would excise the mandate and leave the rest of the act in place,” he said. This suggests the healthcare law could survive even if a part of it is struck down, but the justices are not likely to deliver their final decision until Spring of 2021.
Source: Al Jazeera